Are Family Observations the Missing Link in Palliative Care?

Marcus Stow
Marcus Stow

Family carers are an often-overlooked resource in patient observation, with significant potential to support palliative care teams. Equipping carers with tools to measure and document their observations of the patient provides professionals with valuable insights that enhance clinical decision-making. Such structured family observations can serve as an essential component to capture a fuller picture of palliative patients’ well-being in their home environment. Regular monitoring by family carers improves understanding of a patient’s condition between professional visits. Offering guidance on what to observe and a structured format for recording this information significantly increases its accuracy, consistency, and utility. Mobile technology can further empower carers by providing accessible tools for symptom tracking and support. Apps allow carers to log symptoms, access resources, and generate visual summaries for easy review, which helps structure their routines and supports continuity of care. These digital tools not only assist family carers but also supply essential data and insights to clinical teams, ultimately having the potential to enhance the quality of palliative care.
Providing, supporting, and advising on palliative care are among the most challenging aspects of any community practitioner’s role. Whether you are a General Practitioner, Nurse, Physiotherapist, Social Worker, or Occupational Therapist, the task of communicating with and supporting those nearing the end of life—and their families—comes with unique and complex challenges. These range from helping provide physical care in a completely inadequate environment, through complex symptom management, to supporting general well-being in what can be a dire scenario. In palliative care, symptom presentation may change very slowly or quite suddenly, requiring professionals to frequently monitor, analyse, and adjust to evolving patient needs. This “continuous monitoring and management of a person’s symptoms and performance status [is] vital for the delivery of effective palliative care”.
However, achieving continuous oversight is complicated by the unpredictable deterioration of palliative patients, whose needs for physical and emotional support tend to increase over time. This requires that the palliative care team continuously assess and adjust the patient’s treatment, side effects, symptoms, and overall well-being. This difficulty is exacerbated by the limited frequency with which professional team members can ‘access’ the patient and their family carers. The frequency of access is highly dependent on the patient caseload of community practitioners, which in the UK is usually too large. A high workload also limits the time available for each visit, placing additional strain on the palliative teams who would ideally want more time with patients under their care. The authors of the RELIEF study noted that “the lack of timely symptom reporting remains a barrier to effective symptom management and comfort for patients with cancer-related palliative care needs.” They further observed that inadequate symptom management at home can result in negative outcomes, including increased emergency department visits and, in some cases, in-hospital death.
As we know, a dying patient’s condition can change dramatically in just one week. Therefore, undertaking a full holistic assessment can be difficult in a limited time window, especially if there are new presenting symptoms. The potential result? The professional may not have enough time to take in all relevant information to fully understand: a) what has happened since their last visit; b) how things are right now; and c) any specific patient concerns. Ascertaining the detailed patient need and adjusting their care plan with limited time requires training, experience, and commitment. It can be challenging at best and nearly impossible at worst.
As illustrated in the case example below, the information family carers gather can be invaluable. However, without structure, this valuable resource often goes untapped. As a community palliative care provider, patient visits are likely limited to once a week and often for much shorter periods than you would prefer. Gathering concise and accurate information about the patient’s state, well-being, and health during the intervening period can be extremely challenging, especially in a short visit.
Community care professionals excel at involving patients and family carers in information gathering. However, the collected data often lacks structure, is emotional and anecdotal, and varies from one care professional to another. This valuable information on the patient’s condition is usually very subjective and restricted by a particular carer’s exposure, observational ability, and understanding of the patient and their condition. The accuracy and scope of information provided by the patient depends on many variables, including their ability or willingness to communicate, their mood, energy levels or underlying symptoms such as pain.
Given the limited time and exposure to the patient during visits, it makes sense to bring the family carers into the data collection role in a more structured and planned manner. This is what is referred to as family observations.
As we know, family carers approach their support duties differently from one family unit to another. Some have the time and ability to be very organised, take notes, track symptoms, and report back effectively. Others have limited time, may be very stressed, and may not understand what information could be useful to the professional care team. Providing the family carer with the guidance on taking basic observations—what to look for and when—and the tools for recording them can greatly assist not only in getting useful and structured information, but also in serving as a valuable checklist for care provision itself. For example, having a daily reminder to ‘record pain levels’, ‘catheter output’ or ‘pressure areas’ can act as an excellent prompt to help direct useful activity. When recorded and reported well, these simple observations can form the basis of consistent and valuable feedback to the professional team. Simple checklist-based activities also help with continuity of care, facilitating handover between carers and making it easier to track what has been done and what tasks still need doing. Recording and reporting care activities is essential for medication administration, nutrition, pain assessment, detecting signs of infection, and other aspects of care. Such care observations are illustrated below.
Consider the scenario below, which describes two different outcomes based on how health information is passed from family carers to the professional palliative care team.
Scenario 1
You are on your weekly visit to Mrs. Larsen, who has been under the care of the palliative team for several months. She has gradually become less mobile, her pain levels have increased (with various medication changes), she has a recurrent urinary infection, and she is beginning to have difficulty eating and drinking. Sadly, your time is limited to 30 minutes. Upon arrival, Mrs. Larsen’s sister and daughter begin to barrage you with information about the past week in a hurried, unstructured, and, at times, contradictory manner. You manage a quick assessment of the patient while being verbally updated by the two family carers. Mrs. Larsen states that her pain is “8/10” and cannot recall if she has passed urine recently. Just as you are about to leave, Mrs. Larsen’s daughter mentions, “Oh…she hasn’t been able to take her tablets for a couple of days, and we think she has developed a new pressure sore on her bottom.”
Scenario 2
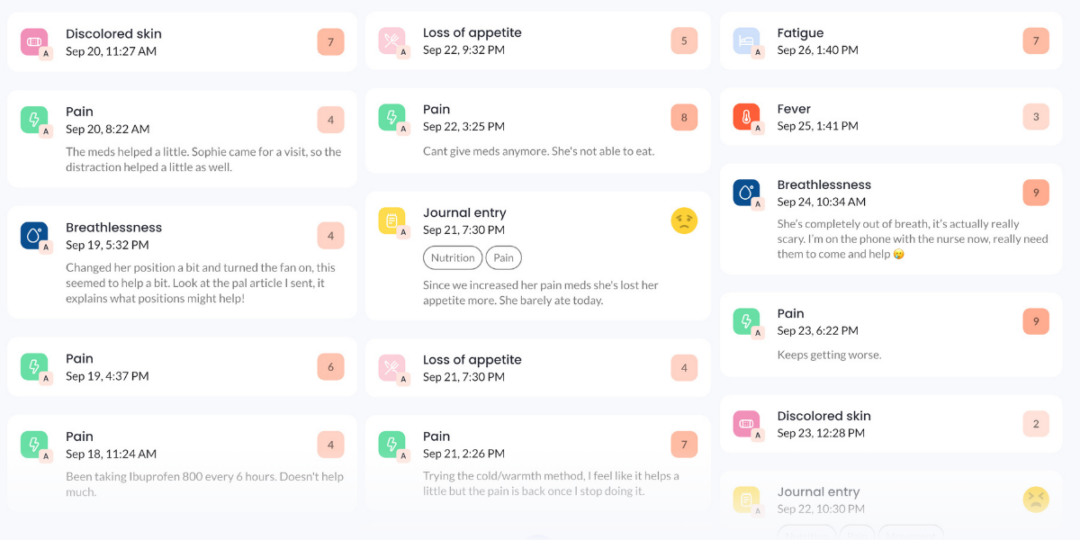
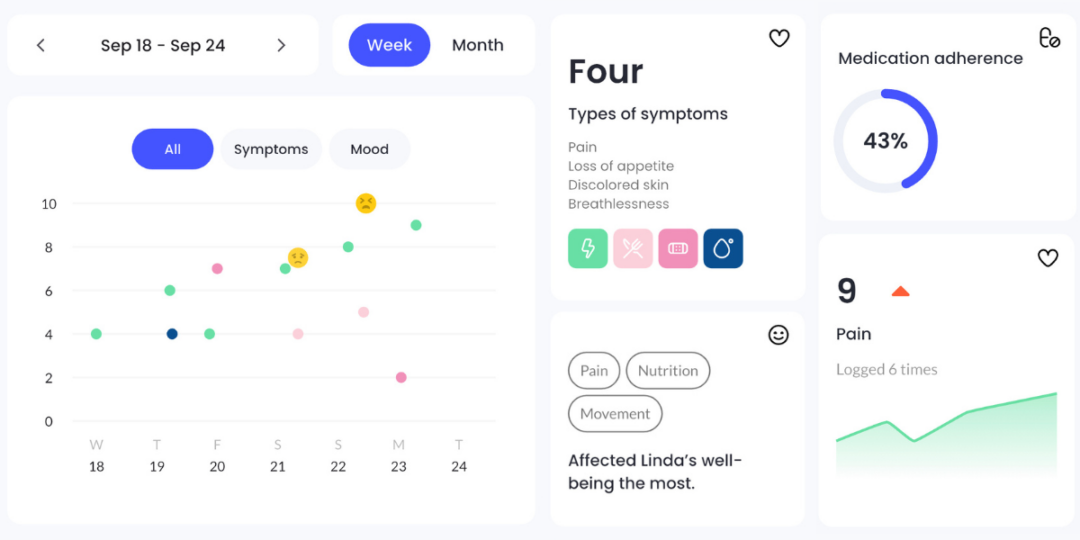
Now, imagine the same scenario, but the family carers have been recording Mrs. Larsen’s progress using an app since she was diagnosed with a life-limiting illness three months ago. Mrs. Larsen’s sister invites you in and shows you the observations summary, with a focus on the past week. You review a dashboard on the app that shows pain has gradually increased over the week, and medications have not been given due to her inability to eat. The family also logged skin redness and have already started providing pressure area support as advised by the app, awaiting further instructions from you during your visit today.
In the past, hand-written notes, chart filling, or list-making would have been advised as common methods for monitoring and recording patient observations. While jotting things down is far better than relying on memory and anecdotal verbal accounts, these notes and home-made lists can still be inconsistent, incomplete and vary between carers. Also, completing written records—even when using a formalised template—can be intimidating, overly complex, and may include observations that are not relevant to a particular patient’s care.
Effectively displaying a patient’s status, care effects, and relevant data is crucial for supporting healthcare professionals. One of the greatest leaps forward in the electronic age is the ability to record, review, analyse, summarise and display data. This has been particularly helpful in healthcare settings. For example, digital platforms like EMIS Web or SystmOne, widely used in UK primary care, allow for the real-time recording and sharing of patient data across multidisciplinary teams, though they are often underutilised in palliative care. Mobile health apps, such as ‘Florence’ (a text messaging platform for remote patient monitoring) or ‘my mhealth’ (which supports patients with long-term conditions), demonstrate how technology can enhance data collection and patient monitoring. Despite being widely recognised as a clinical game-changer, the NHS has been slow to develop or adopt widely available technologies that allow the collection of detailed, comparable and ‘cleansed’ (i.e., the process of fixing or removing incorrect, corrupted, or incomplete data) data. Furthermore, it is safe to say that the NHS has not always been able to utilise its current data in ways that directly benefit clinicians or patients.
The rapid onset of Covid-19 and the consequent SARS epidemic led to a swift advancement of electronic physiological and symptom data collection in the community, starting with the distribution of SaO2 finger probes and the remote monitoring of respiratory function. Patients were able to record and self-report their blood oxygen levels and any associated symptoms. During a time when hospital beds were at a premium, this new method of monitoring patients reduced hospital admissions and readmissions. By enabling data collection in the community, secondary healthcare providers were better able to focus on the acutely unwell and swiftly triage patients at home. The utility of symptom collection technology was further enhanced by combining it with telemedicine software, leading to the development of the ‘Virtual Ward’ concept, an adaptation of the ‘Hospital at Home’ model of care. Telemedicine has also been successfully used in palliative care settings with positive results—as an adjunct, not a replacement, to face-to-face visits. In the last five years, these community-based observation and response care systems have become more widespread, providing monitoring, observation, advice and treatment that is not restricted to the inpatient hospital or hospice setting.
Over the past decades, many advanced mobile apps and software systems have been developed to support health and well-being. Often connected to sensors like watches and rings, most are produced by large corporations and operate on a subscription or advertising model. These apps primarily aim to maintain and promote health in healthy individuals rather than assist in care or treatment. However, some condition-specific apps, such as those for diabetes, have significantly improved disease management by offering health promotion information and structured methods to track metrics or symptoms. There are very few software systems designed specifically to support palliative care in the community and none that are being used extensively. Palliative care-focused apps present a huge opportunity for better oversight, informed treatment, and continuity of care in the community.
An app can provide swift access to collated, focused advice, link to educational resources, and guide the user to other educational material they may need. An empowered family carer using this kind of care assistance tool can be guided to input simple observations, be educated on how and what to observe, and use a structured method to record patient health information.
Using a digital tool or app can provide a structured routine for the carer, help track progress, aid handovers between carers, and boost continuity of care. For the professional palliative care team, access to a formatted and easily reviewed symptom dashboard can undoubtedly assist with and expedite care assessment and dynamic decision-making. Using focused palliative care software increases the accuracy, consistency and utility of any information provided by a family carer to the professional palliative care team.
In conclusion, empowering palliative family carers to gather and record patient observations in a digital format is a simple, cost effective, and powerful way to enhance professional interactions. It not only improves the quality of care but also strengthens family engagement and positively impacts the patient’s palliative journey. As healthcare continues to evolve, embracing digital tools in community care settings is not just a forward-thinking strategy, it is a necessary step towards ensuring that palliative care is as responsive, personalised, and effective as possible.
Written by Marcus Stow
Marcus is a compassionate nursing officer and clinical leader with over 20 years of experience.